In This Article
- Why Triage?
- Assessments
- Dead and Dying
- Check and Check Again
- Methodically Engage Chaos
- The SALT Method
- 1. Beware of the Box
- 2. Denote the Dead
- 3. Remember Your ABCs
- 4. Plan on Changing Your Plan
- 5. Tourniquets: High and Tight
- Pro Med Kit
- Triage and Treatment Gear Review
- Suggested Training
- Conclusion
- About the Author
- More From Issue 18
You’re at a football game when shots ring out. A lot of shots. Then screams. You know instantly this is a mass-shooting scenario, and you want to help after the smoke clears. Though developed by the Centers for Disease Control and Prevention (CDC), the Sort Assess Life-saving Triage (SALT) method can be used by anyone to help save lives before first-responders arrive.
As a prepper, you might think, I’m no paramedic. How can I use SALT after the shooting stops?
Although many people think “mass shooting” when they envision a mass-casualty incident, by definition it simply means that there are more casualties than can be effectively managed by the available resources. There doesn’t need to be dozens or hundreds of victims. Two paramedics pulling up to the scene of a school bus crash just walked into a mass-casualty incident. Six victims of a gas leak explosion at a mountain cabin, treated by one lone hiker with an individual first-aid kit (IFAK), would be classified similarly.
Why Triage?

Triage is a decision scheme designed to help medical responders use their limited resources in a way that benefits the most people. In a situation where scores of people have been hurt, devoting time and supplies to a victim who will soon die or to someone else who’s barely scratched are equally bad decisions at opposite ends of the spectrum. The goal is to devote resources where they are most needed and most effective.
So how do you figure out who gets helped first? Start by sorting them. Those who are able to do so need to walk, stumble, or crawl to a nearby location of your choosing. You could say, “If you can hear me, I need you to move to the other side of this area. Do it now.”
This one simple statement may be the most important factor in deciding who gets helped first. It can instantly separate those who can more or less help themselves from everyone else. Anyone who just moved is able to hear and understand, and their body is still (mostly) functioning. This means they can be put out of your mind, at least for now.
Assessments
Those who are still on the ground need to be looked at more closely. They can be subdivided further by calling out a second command: “If you can hear me, I need you to wave your hands. Do it now.” If you can see purposeful movement on their part, they’re probably not the ones who need treatment first. The ones who need to be looked at immediately are those who were still unable to respond.
At this point you’ll have discerned up to three categories of victims: the “walking wounded” have been triaged as minimal and would be coded green. Those who can obey your commands and don’t look too messed up can be coded as yellow, denoting delayed care. The remainder, who need urgent life-saving intervention, are coded red because they need immediate care.
Dead and Dying
Confirmed dead would be coded as black, and should be moved to a separate area as time allows. This will help reduce the likelihood of late-arriving responders wasting time assessing those who are beyond help. For example, at the Virginia Tech mass shooting in 2007, some deceased victims were inadvertently rechecked three or four times, diluting vital resources.
There’s also a fifth category called expectant, which is coded gray or black-and-white. If a victim is coded as expectant, it means their injuries are so severe that they’re probably going to die because there aren’t enough available resources to meet the demand. For this reason, no care should be provided to them until more urgent cases are addressed. If and when resources become available, an expectant patient could be upgraded to the priority red category.
The expectant category hasn’t been widely adopted within the EMS community throughout the United States. The term is familiar to those working in the U.S. Department of Defense, but has only recently become part of the civilian EMS vocabulary with its use in the SALT triage system.
Check and Check Again
Keep in mind that triage isn’t a one-and-done event. It’s a dynamic process that changes based on the condition of your patients, your available resources, and scene safety. For example, once priority (red coded) patients have been treated, they may be upgraded to delayed (yellow). If a delayed patient has a cardiac arrest while you’re working on someone else, they may be downgraded to expectant. Their treatment priority will also change as the most urgent (and transportable) victims are evacuated, freeing up resources for the remaining patients.
Methodically Engage Chaos
Knowing the theory is great. So is having a plan. But as former heavyweight champ Mike Tyson put it, “Everybody has a plan until they get hit. Then, like a rat, they stop in fear and freeze.” What matters most is being able to methodically engage chaos, rapidly make difficult decisions, and improvise using only the resources at hand. With this in mind, we spoke to Sean McKay, the director of Disruptive Rescue/Austere Medicine at Element Rescue and program manager of Mobile Training and Rescue Development at Rescue Craft by Tactical Medical Solutions.
Although a firefighter and SWAT paramedic in his past life, McKay now spends his time developing dynamic rescue training and specialized products for elements of the U.S. Special Operations Command and federal assets, among other organizations. We asked him how civilians could effectively use triage theory in their own lives based on what has worked (or failed) in the past.
“First of all,” McKay says, “understand that many organizations within special operations usually don’t use a rigid algorithmic response like the SALT system. Those were designed for first responders, EMS units, and hospitals with layers of known resources to call on.
“When the excrement makes physical contact with the rotating blades, civilians would never remember all the little details in the heat of the moment. Instead, they need to use common sense and trust their gut. “Usually your gut assessment is correct,” McKay says. “There are three categories of patients you may encounter. First, those who will die no matter what you do. Second, those who will live no matter how bad you suck. And last, those who have a potentially preventable cause of death that you can impact. Focus on them.”
The SALT Method
Sort Assess Life-saving Triage
(Note: Users of any triage system should only apply lifesaving interventions up to the level of their training and expertise.)
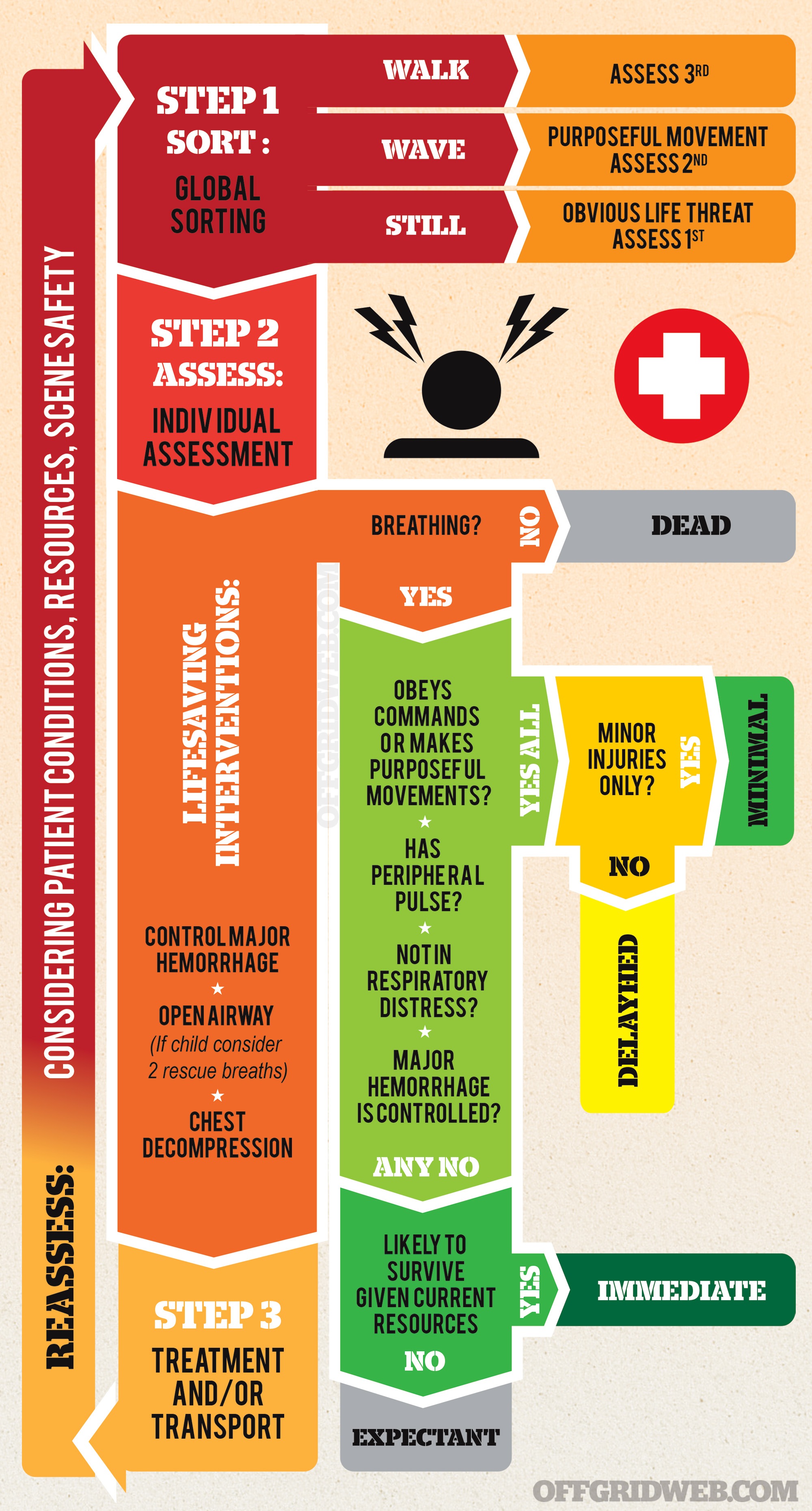
Source: U.S. Department of Health & Human Services REMM – www.remm.nlm.gov
Readers would also do well to heed these five additional tips from McKay:
1. Beware of the Box
If someone can talk to you, that means they can breathe. Move on. But if someone has a penetrating wound in “the box” (from their belly button up to their collarbone) they should become a priority for transport when available.
Injuries to this area are often complex for the caregiver for a few reasons:
- The patient can decompensate (start dying) quickly because all the vital organs are located in that region.
- There isn’t much a responder can really do besides cover a sucking chest wound or (for the advanced care provider) decompress with a needle.
- “For the non-medical person, it’s hard to appreciate relevant versus irrelevant breathing pathology,” McKay says. In other words, their breathing may sound like they’re dying, but they’re actually just scared. The patient could be breathing fast due to exertion, pain, stress (flight or fight), or could have a life-threatening issue with blood or air filling up their chest. “Keep your breathing assessment simple,” McKay says. “Copy their breathing pattern and speed. If it’s uncomfortable for you, it’s even worse for your patient.”
2. Denote the Dead
Move the dead away from the living (if tactically feasible) and provide a visual cue to other bystanders or first responders that you have triaged the casualty. Professionals may use colored electrical tape or casualty cards to mark the victims. Or better yet, copy what some British elements do — roll the victims face down and cross their arms and legs. This will prevent re-triaging and is faster than taping or marking.
3. Remember Your ABCs
“Blood goes ’round and ’round and air goes in and out,” McKay says. “If there’s an interruption, it needs to be addressed.”
Airway, breathing, and circulation used to be what first responders checked on a victim, and in that order. Then somewhere along the way we figured out that victims can get oxygen back once they start breathing again, but they can’t get back blood. And they can bleed out a lot faster than they’ll die from lack of air. This means that the new method is to check the patient’s circulation, breathing, and airways, in that order. Blood spraying into your eyes is a good indication that you found the right place to get to work.
Since irreversible shock and death can occur within three minutes from a femoral artery injury, bleeding control (B-con) should be the life-saving intervention that you focus on. Any uncontrolled bleeding, especially from an extremity, needs to be managed immediately.
4. Plan on Changing Your Plan
You will run out of supplies, so you must know how to improvise materials. Need a soft litter to carry or drag someone out? Lay the victim down on a carpeted floor and cut with your knife around the outline of the patient, staying about 8 inches off their shoulders. Then cut a few slots down each side about 4 inches in from the edges for handles.
Or if you need a tourniquet and you understand how a tourniquet works, you can make one out of anything. “If I walk into a room and see three picture frames on a wall and each one has four corners, that means I have 12 windlasses for tourniquets,” McKay says.
5. Tourniquets: High and Tight
Don’t worry about cutting off their clothes until you have time to check for secondary injuries. “If you look and see blood spraying from their legs or arms, or blood-soaked clothing, just get the tourniquet up on their limb as high as possible,” Sean says. “It will still be effective over the clothing as long as it’s properly applied.”
And how does one know if it’s properly applied? “The tourniquet should feel like it’s f*cking killing them,” he says. “It should go beyond the point to where it’s tight enough that they know it’s there, to the point where the pain of the tourniquet is all that they’re thinking about … and it’s not bleeding anymore.”
Keep in mind that the tourniquet can easily remain in place for up to two hours without risk of permanent damage. So don’t get any funny ideas about loosening it a little bit once in a while to make the patient more comfortable. That’s a good way to kill a patient.
Pro Med Kit
A former firefighter and SWAT paramedic, Sean McKay is the director of Disruptive Rescue/Austere Medicine at Element Rescue and program manager of Mobile Training and Rescue Development at Rescue Craft by Tactical Medical Solutions. Here’s what he carries in his med kit and why:

Multiple SOFTT-W Tourniquets: “These are one of the most widely used tourniquets within U.S. Special Operations Command and large city first-responders,” McKay says. “They’re known as the AK-47 of tourniquets because they’re so durable. You can treat that thing like a prison bitch, and it’ll keep working regardless of environmental factors.”
Chest Seals: These are needed to treat sucking, penetrating chest wounds. McKay also carries a sturdy decompression needle to vent the chest and prevent a buildup of air within the chest cavity. Lesser-trained civilians should focus on simply being able to “burp” the wound by lifting the seal, instead.
QuikClot Combat Gauze: “I choose Combat Gauze specifically,” he says, “because it has been tested and evaluated to produce the most robust clot, and maintains 0-percent re-bleeding within all the patient movement studies. Other similar products have been shown to open up and cause re-bleeding when the patient is being moved — in some products it’s over 30 percent.”
“Like many, I have a med/rescue response bag in my vehicle, but when going around town or traveling out of town or on a plane, I always have a SOFTT-W, a Combat Gauze, an elastic Esmark bandage, and a plan to improvise the rest.”
Triage and Treatment Gear Review

Bag: Specialized products for mass-casualty incidents (MCI) are now making their way to the mainstream. The TacMed Warm Zone sling bag from Tactical Medical Solutions is among the best, having been designed from the ground up for medical personnel who need to stay mobile while treating and triaging victims. Its pull-and-place modular interior system allows medics to customize the layout that suits them best. It comes stocked with an MCI loadout, including tourniquets, casualty marking tape, bandages, and marking pens, among other items. www.tacmedsolutions.com
Light: We were always taught to store our flashlights with the batteries reversed, to avoid long-term corrosion of the terminals and accidental turn-ons. That theory is sound, until you need a light source in a hurry and your fine motor skills aren’t what they were 2 minutes ago before the bomb went off. For this reason, we love the new FL75R headlamp from Coast Products. The dual-power system can run on standard alkaline batteries or its included micro-USB powered rechargeable pack. This lets you keep it plugged in so it’s always charged, while keeping loose AAA batteries on-hand for when extended use is required. www.coastportland.com

Everywhere-Everytime Med Kit: The TacMed Pocket Medical Kit is similar to the full-time med loadout described by Sean McKay of Element Rescue in the sidebar found elsewhere in this story — the one he carries on him even if he can’t carry a bag. Stripped down to the bare essentials for bleeding control, the kit is small enough to fit into the back pocket of your jeans and includes a tourniquet, Esmark Bandage, Combat Gauze, chest seal, and gloves. www.tacmedsolutions.com

Bag or Trunk Med Kit: The Tramedic Individual Response Pack by Griffin Logistics is a larger, upgraded kit that can be stored in a medium-sized purse, backpack, or trunk of your vehicle. It includes a bleeding control loadout similar to the pocket kit noted above, but also packs in some extras that could make a long day much easier for you. This includes material to maintain an airway for an unconscious person, as well as a clever (and much more likely to be used) Minor Injury Kit with adhesive bandages, tape, forceps, and antibiotic ointment among other items. Griffin’s gear is the real deal, and it shows in the look and feel of their products. Look for their trauma kits to start showing up in stadiums and concert venues, in wall-mounted cabinets next to the defibrillating AED devices. www.griflog.com
Suggested Training
For in-person classes that civilians can attend, check out the National Association of Emergency Medical Technicians’ website at www.naemt.org/education.aspx. You can search for upcoming sanctioned classes near you. This may include Tactical Emergency Medical Care (TEMC) as well as Bleeding Control for the Injured (B-Con), which is a simplified course designed specifically for non-medical personnel.
Also look for Tactical Combat Casualty Care for All Combatants (TCCC-AC), which is designed to introduce basic battlefield medical treatment to non-medical responders.
Online training can be obtained by watching videos at the following websites:
Element Rescue
www.elementrescue.com
North American Rescue
www.narescue.com/training/videos
Tactical Medical Solutions
www.tacmedsolutions.com/training-resources
Conclusion

Whether the event is a plane crash on a remote mountainside, a Boston Marathon-type bombing inside a city, or the mass shooting that seems to be on everyone’s minds, the triage process will work the same way. “Principles stay the same regardless of environment,” McKay says. “It all comes down to the laws of medicine and physics, and how you manage them.”
Sources
U.S. Department of Health and Human Services
Radiation Emergency Medical Management
www.remm.nlm.gov
“Mass Casualty Triage: An Evaluation of the Science and Refinement of a National Guideline”
Journal of Disaster Medicine and Public Health Preparedness
https://www.cambridge.org/core/journals/disaster-medicine-and-public-health-preparedness
About the Author

Andy Schrader is a licensed professional engineer and certified by the U.S. Army Corps of Engineers as a structural specialist responder. He is assigned to Urban Search and Rescue (USAR) Task Force 8, based in Marion County, Florida. His company, Recon Response Engineering, teaches the public, technical rescue teams, and other first-responders about structural collapse. Most recently he was deployed to Steinhatchee, Florida, in support of SAR operations following Hurricane Hermine. www.reconresponse.com / www.facebook.com/ReconResponse
More From Issue 18
Don’t miss essential survival insights—sign up for Recoil Offgrid’s free newsletter today!
- Cold War Combatants: Essential Preps for Winter Driving
- The Hills Have Eyes: Tips for Camping Safely Near Dangerous Game
- Improv Skills: Using 5 Common EDC Tools as Improvised Weapons
- The SALT Method: Triage and Treatment for Mass-Casualty Incidents
- What If You’re Trapped in a Mass Shooting?
- Fire at Will: Fire-Starter Buyer’s Guide
- Covering Your Assets: Legal & Financial Prepping
- How to Survive a Mass Shooting While Unarmed
Read articles from the next issue of Recoil Offgrid: Issue 19
Read articles from the previous issue of Recoil Offgrid: Issue 17
Check out our other publications on the web: Recoil | Gun Digest | Blade | RecoilTV | RECOILtv (YouTube)
Editor’s Note: This article has been modified from its original version for the web.

 method can be used by anyone to help save lives before first-responders arrive.){kind=link}