In This Article
This article was originally published in Issue 1 of our magazine.
WARNING: This article is meant to be a quick overview and not a detailed guide on procedures relating to the treatment of puncture wounds. To be prepared for any emergency, we encourage you enroll in a certified medical course or, at minimum, a familiarization course, which will deliver comprehensive knowledge of how to treat different types of puncture wounds.
The unfortunate reality is that injuries may occur to you or those around you at anytime and without warning. One such type of injury is a puncture wound. How you deal with a wound of this kind and how quickly it is dealt with can save a life, allow time to get someone to safety, or at least prolong the victim’s survival time for help to arrive.
The definition of a puncture wound is: “A traumatic injury caused by skin penetration by an object, such as a knife, nail, or slender fragment of metal, wood, glass, or other material that does not move laterally from the point of entry.” Puncture wounds come in various forms and severities. A post-disaster urban environment is fraught with dangers that can contribute to puncture wounds. Fallen debris, broken glass, and exposed rebar are just a few of the dangers in which you could be accidentally injured. More lethal manmade varieties of puncture wounds, including wounds caused by a bullet, a knife, or an arrow are hazards you should be prepared to deal with, as well.
The severity of a puncture wound greatly dictates the actions that should be taken. Some minor wounds that are non-life-threatening can be treated in the field, using basic supplies that allow the patient to be stabilized for long periods of time. Other wounds can be very traumatic, making it imperative that the patient receives more advanced care. The goal in the field is to provide treatment to extend the survival time of the patient until proper help can arrive.
“The Golden Hour”
The human body has the remarkable ability to compensate for many types of injuries in order to keep the body alive. Despite its best efforts, the body can only compensate for so long and its ability to do so is dependent on the severity of the injury. Emergency medical personnel generally have one hour, which is referred to as “the golden hour,” after a wound is created to stabilize patients and reduce the amount of trauma to the body for the best chance of survival. When treating a puncture wound, remember that time is of the essence, so fast action is imperative. If the proper decision is made for the type of treatment in relationship to the type of injury, survivability may increase.
First, Gather Information
If you come across a situation where you need to treat a puncture wound, there are a few pieces of information you need to determine first before proceeding with treatment.
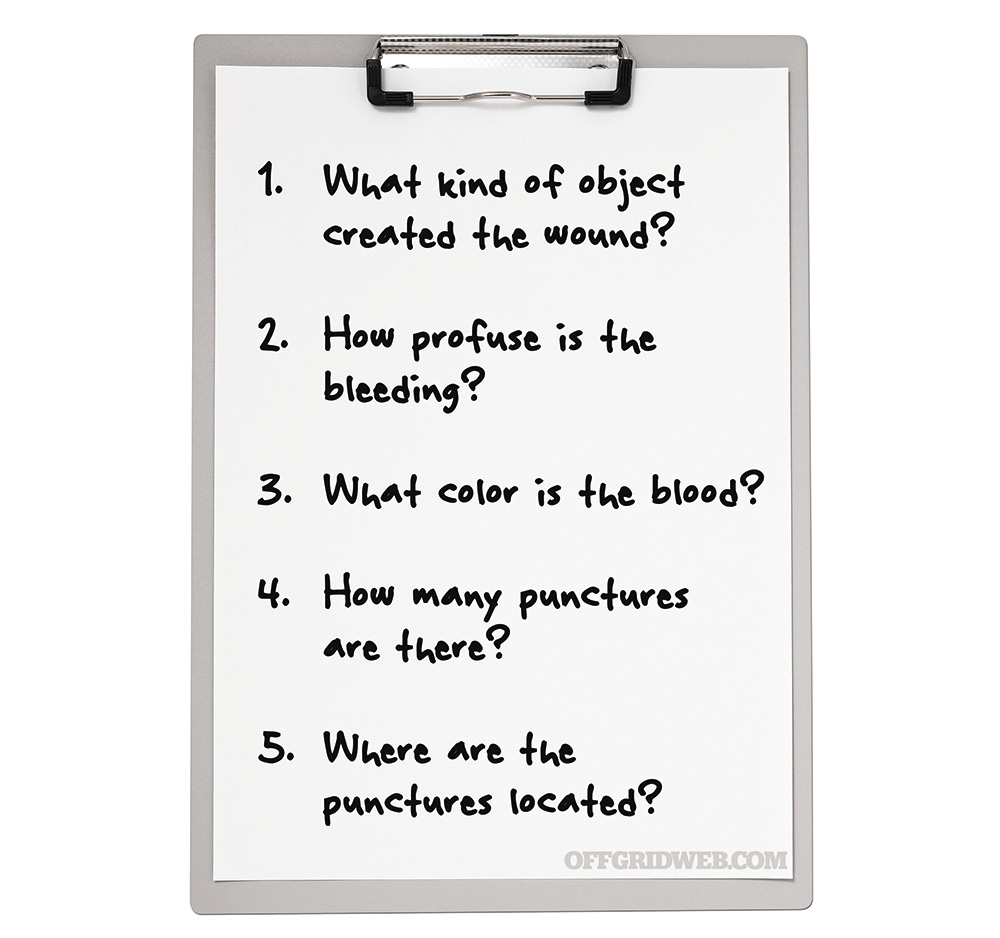
Wounding Object Depending on what kind of object that created the wound, you will either need to carefully remove it or leave it in. If it is easily removed, carefully remove the object from the victim. If it is something, such as a serrated knife, that might create more harm by its removal, then leave it in. However, when in doubt, leave the foreign object alone and bandage around the object.

Blood Loss
Most puncture wounds will not result in massive blood loss. Application of direct pressure followed up by a proper bandaging job should stem the blood flow until further care can be given. If massive blood flow is experienced, then a tourniquet might need to be employed, as well as a hemostatic agent. We go further into tourniquets later in this article.
Bleeding
There are three types of bleeding that can occur, depending on the situation and location of the injury to the body.
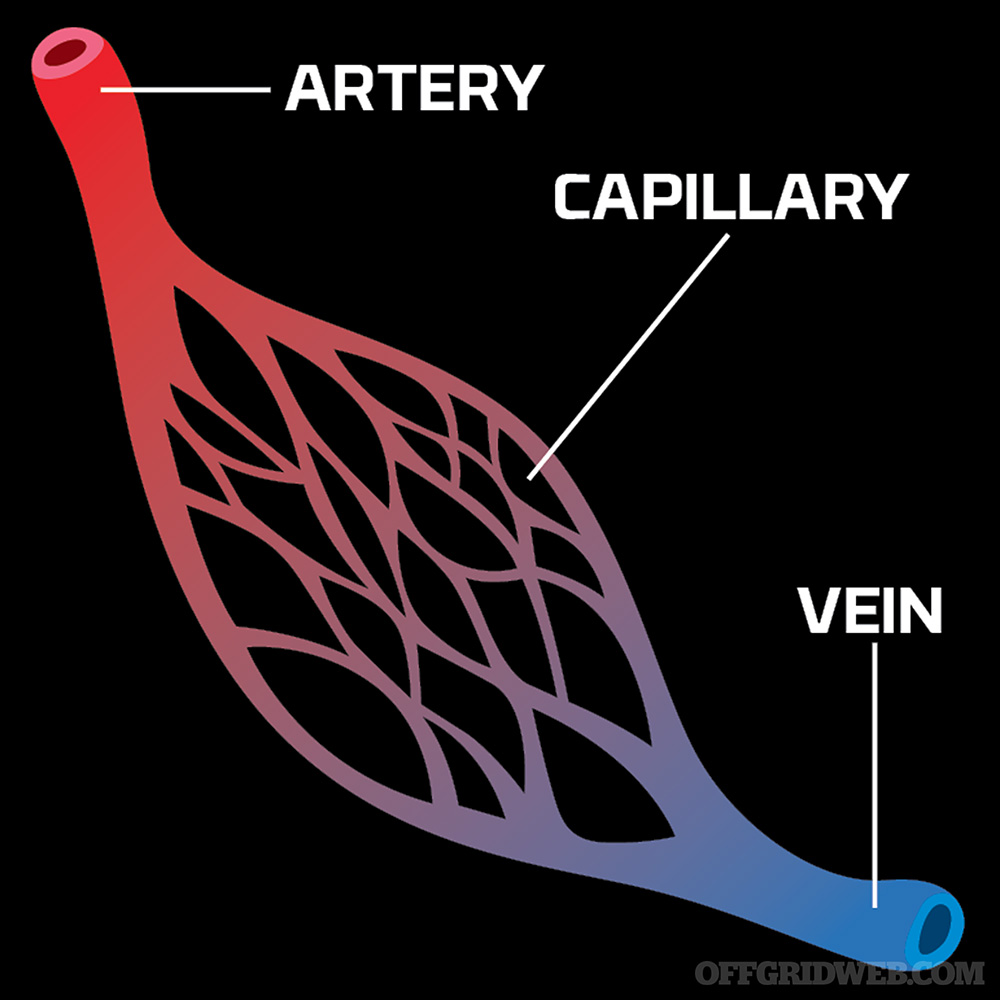
1. Arterial bleeding occurs when an artery is damaged. The blood is under high pressure, and the bleeding that occurs will be bright red in color. This type of blood being under high pressure will cause spurts with every heartbeat. Blood loss with this kind of bleeding is profuse and needs to be stopped as soon as possible.
2. Venous bleeding happens when a vein is punctured and is more of a steady flow of blood that is under low pressure. This blood is darker in color and will have a steady flow. Don’t be fooled, because blood loss from this kind of low-pressure bleeding can be quick, and fast action is required.
3. Capillary bleeding oozes from the wound and is under low pressure. If you have ever skinned your knee or cut yourself shaving, you have experienced capillary bleeding. The blood that comes from this kind of injury is bright in color, but is mostly superficial and not life-threatening.
Number of Punctures
In some cases, puncture wounds can have an entrance and exit place on the body. Not all projectiles causing puncture wounds will simply enter the body and stop. You may have to stop the bleeding in 2 or more places. You must be prepared for more than one area of damage to the body.
Puncture Location
Wounds to most extremities such as hands, feet, arms, and legs can be taken cared of with basic treatment, as long as the punctures do not hit any arteries. When dealing with this particular type of injury, simply applying direct pressure, using gauze, and wrapping the wound, or using a pressure dressing, will usually stop the bleeding. In the event the bleeding does not stop and the first bandage soaks through, then a tourniquet may need to be applied.
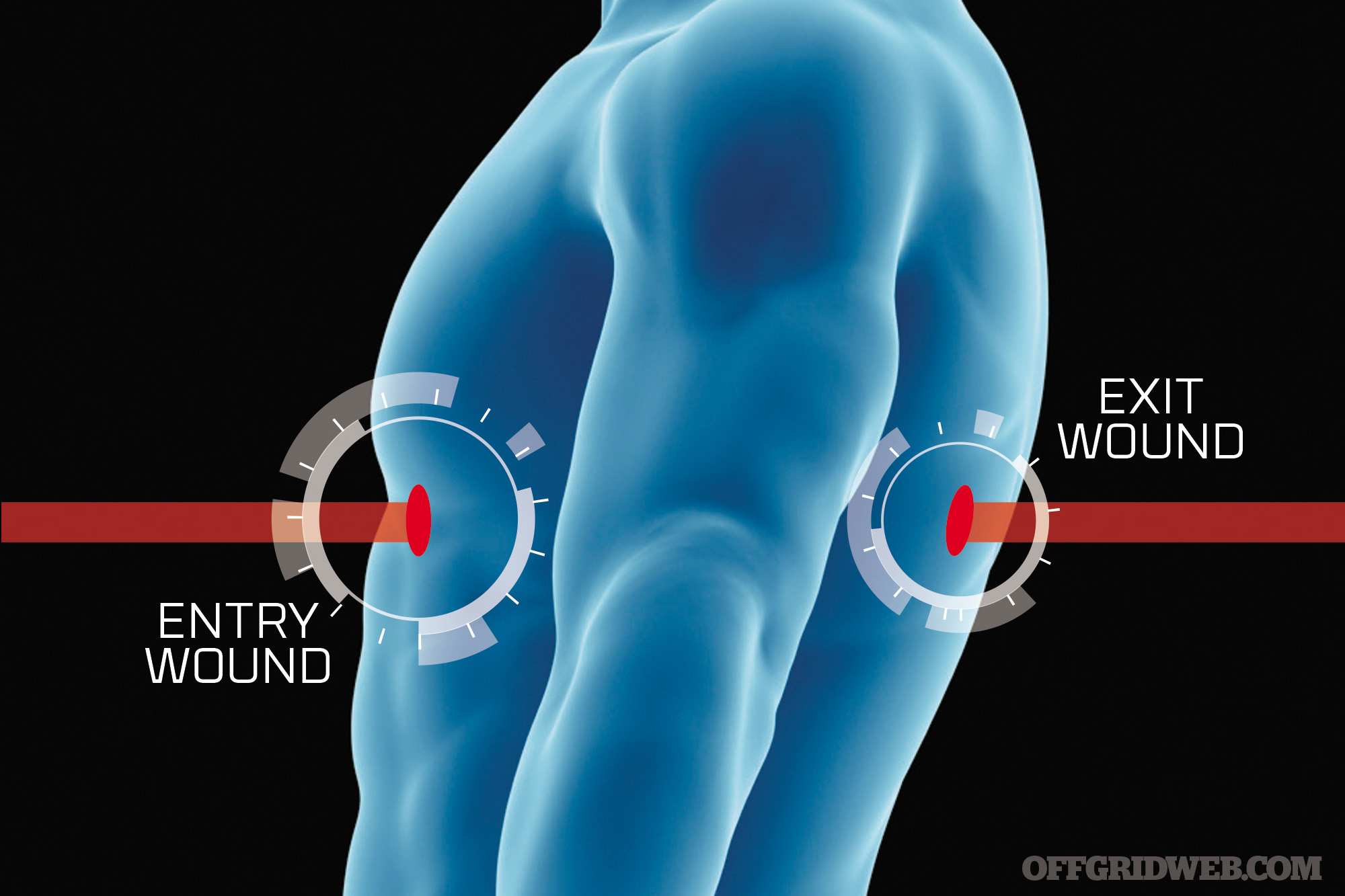
Above: Not all projectiles causing puncture wounds will simply enter the body and stop. Some puncture wounds can have an entrance and exit point on the body.
The Basics of Treatment
First and foremost, the following treatments are temporary and only delay the loss of blood until proper help can arrive. Call emergency services as soon as possible, if these treatments need to be administered. Although there are many variations for the treatment of puncture wounds, the basic idea is to stop the bleeding.

Above: Wounds to most extremities such as hands, feet, arms, and legs can be taken cared of with basic treatment, as long as the punctures do not hit any arteries.
The following steps can achieve stopping the bleeding, but an extreme amount of blood loss occurring may dictate you go directly to the use of a tourniquet.
- Direct pressure
- Pressure bandages
- Tourniquets
- Hemostatic (clotting) agents
Direct Pressure
Applying direct pressure to most puncture wounds will help slow or stop the bleeding. Placing a sterile barrier between your hand and the wound, such as gauze or a bandage, helps reduce the risk of infection. Wearing a protective latex-style glove is ideal. Keep pressure on the wound until bleeding stops. If it does not stop, apply a pressure bandage.

Above: Applying direct pressure to most puncture wounds will help slow or stop the bleeding.
Pressure Bandages
Pressure bandages compress the wound to help slow or stop bleeding to allow for clotting. Adhesive-backed pressure bandages are for application on areas such as the chest or the hand, while rolled bandages can be wrapped around wounds on limbs or the head. Gauze should be placed between the bandage and then wound to help soak up excess blood prior to applying the bandage. If bleeding continues, add more bandages, but do not remove the soaked bandage. If bleeding does not stop after multiple applications, the next step is to apply a tourniquet.
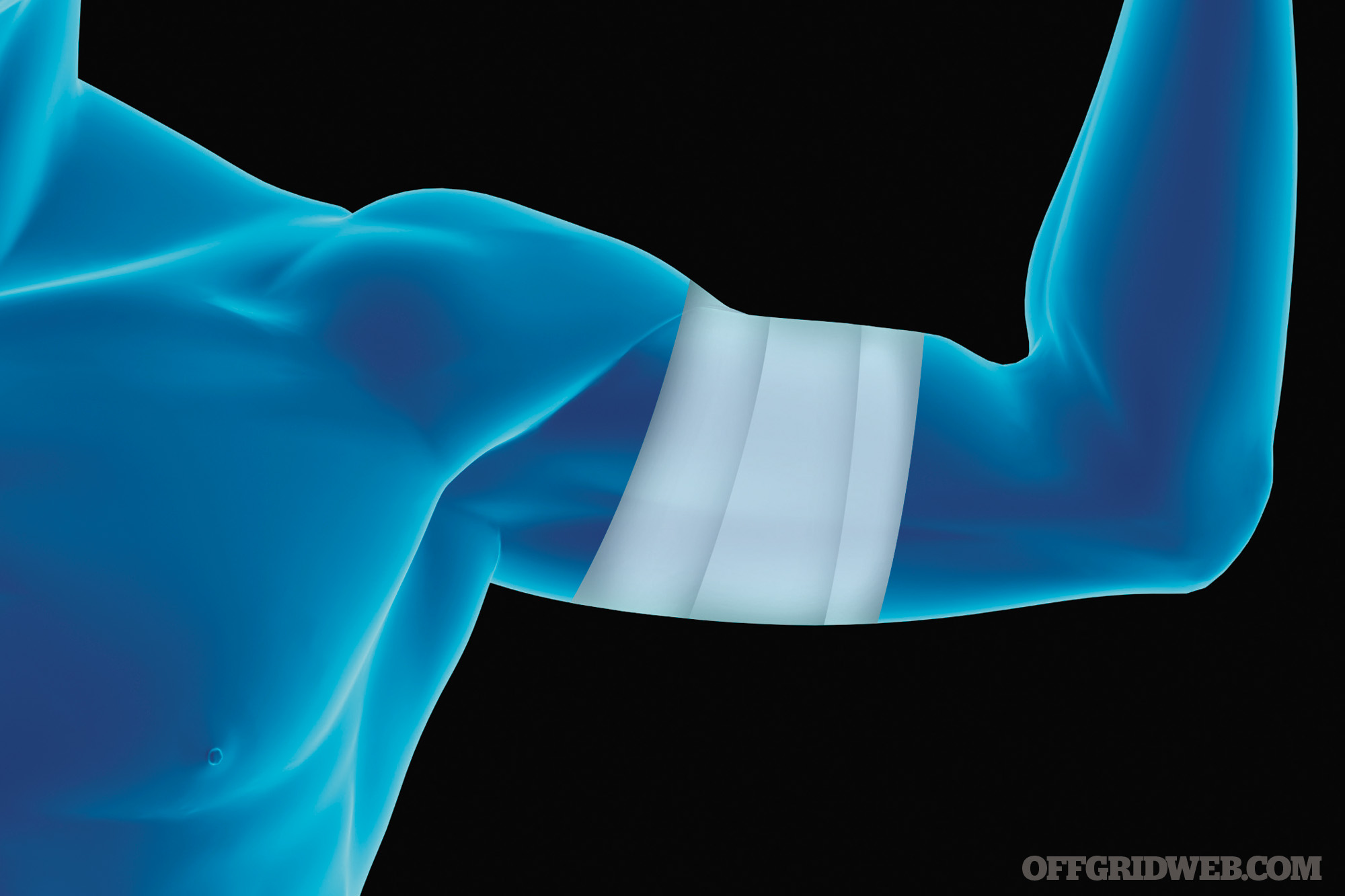
Above: Pressure bandages compress the wound to help slow or stop bleeding to allow for clotting.
Tourniquets
Tourniquets are deployed to stop excessive bleeding from a limb wound. They should be thought of as last resort options, since they completely stop blood flow to the limb and can result in the limb tissue dying, forcing an amputation of the limb.
There are four primary areas to apply a tourniquet: the brachial arteries (arms) and femoral arteries (legs). The objective and placement of the tourniquet is to get it as close to the core or torso as possible. You must apply the pressure in such a manner that the hose or artery is compressed against a bone. When you apply the tourniquet, the objective is to apply pressure and maintain that pressure until the blood flow slows to a minimum or ideally stops the blood loss from occurring any longer.
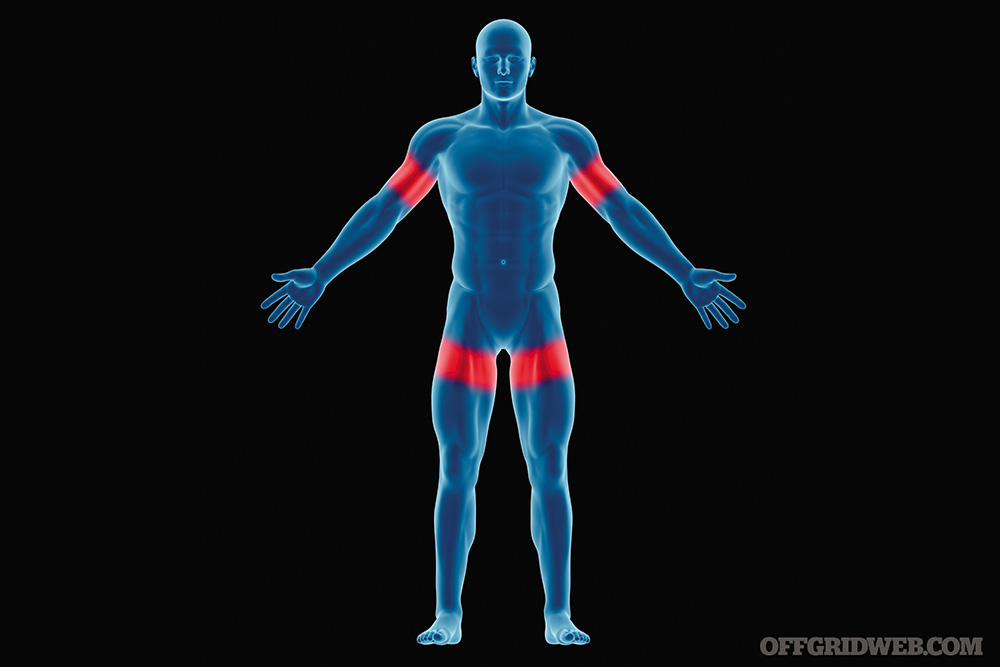
Above: There are four primary areas to apply a tourniquet: the brachial arteries (arms) and femoral arteries (legs).
Remember, a tourniquet is not to be used to stop bleeding from the head, the neck, or the torso and is to treat the major loss of blood from the extremities only. It is better to lose a limb than lose your life in worst-case situations.
Hemostatic Agents
Hemostatic, or clotting, agents should be used based on severity. If in the event that the injury is severe enough, high-pressure blood is being discharged from the body and applying a tourniquet is not completing the job, then a combination of a tourniquet and a hemostatic agent should be used. If there is no tourniquet available, but you have a hemostatic agent, then the agent becomes the first line of defense with some sort of a pressure bandage working in conjunction.
Improvised Supplies
Bandages: Tear up any kind of material, such as clothing, towels, or sheets, to use for bandages if proper bandages are not available. Clean strips of cloth are important, but when in a pinch, use whatever you can to stop the bleeding.

Tourniquets: A belt can be used as an improvised tourniquet in a pinch, or anything wide and flat that can be wrapped around an extremity.
Special Situations
Chest Wounds
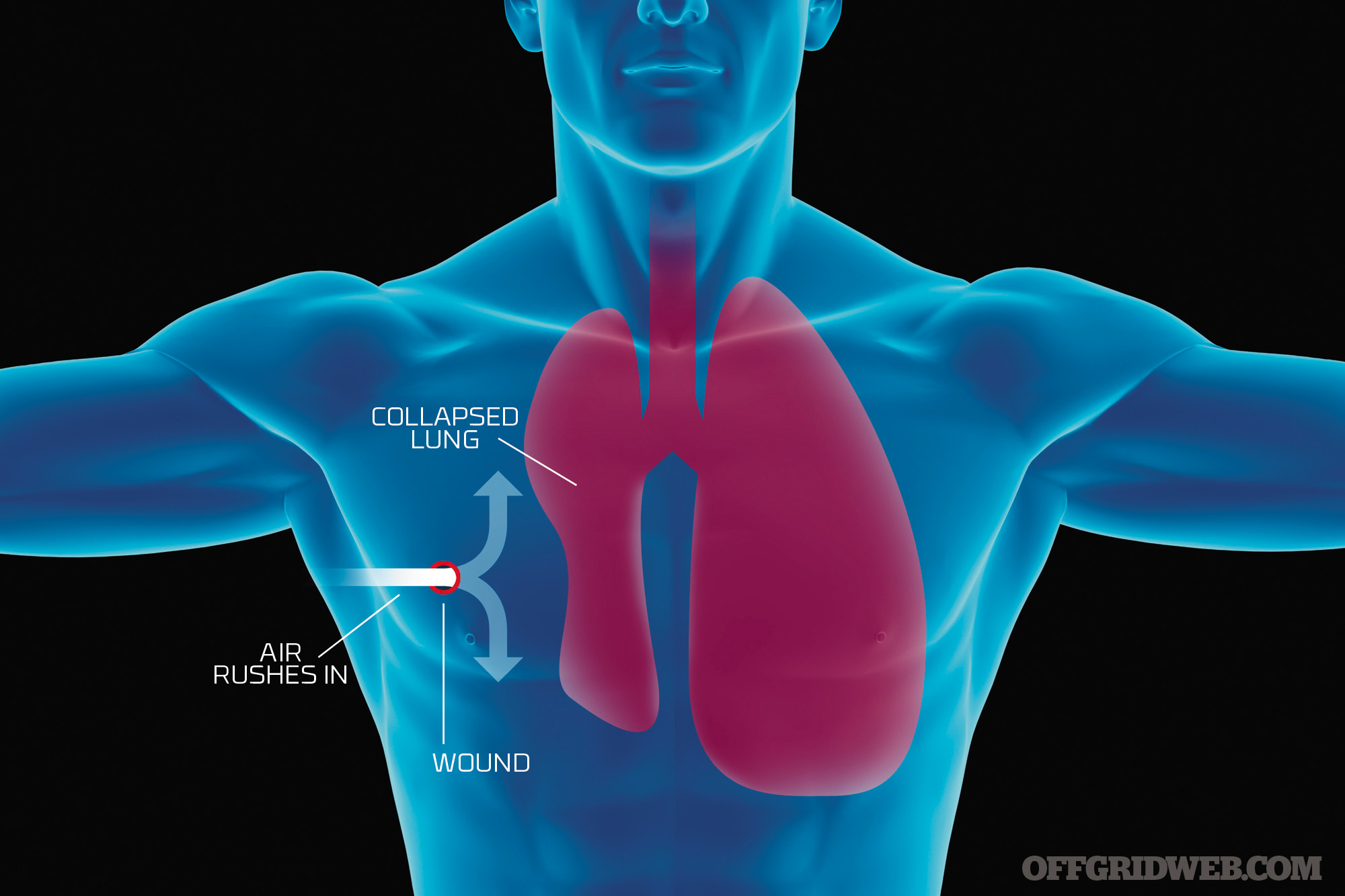
Puncture wounds to the chest region may be more difficult in nature as the type of wound could affect the lungs or even the heart. If you’ve seen the movie, Three Kings, you might be familiar with the segment of the movie where they show a penetrating wound from a bullet that resulted in a “sucking chest wound.” A sucking chest wound is no bueno! As time goes, air enters the chest and starts to compress the lung resulting in a pneumothorax, which is the phenomenon of excess air creating space between the lung and chest wall which makes normal breathing difficult to impossible.
Head Wounds
This is one of those areas that are very hard to assess and treat. The only true life-saving technique is to apply direct pressure and quick transport to a hospital. Any object that punctures the head must be stabilized in the position found, so do not remove it. A trauma center is the only possibility that will save this person’s life.

Simplified Treatment
Without getting into too much detail and any form of advanced treatment, the objective is to apply an occlusive dressing to the chest area that has been subject to the wound. If this wound is in fact a sucking chest wound and if there are obvious signs of labored breathing, such as air bubbles and blood coming from a hole, then the occlusive dressing should be applied. The military is currently employing HALO chest seals. This is a large piece of clear plastic material with a very strong adhesive.
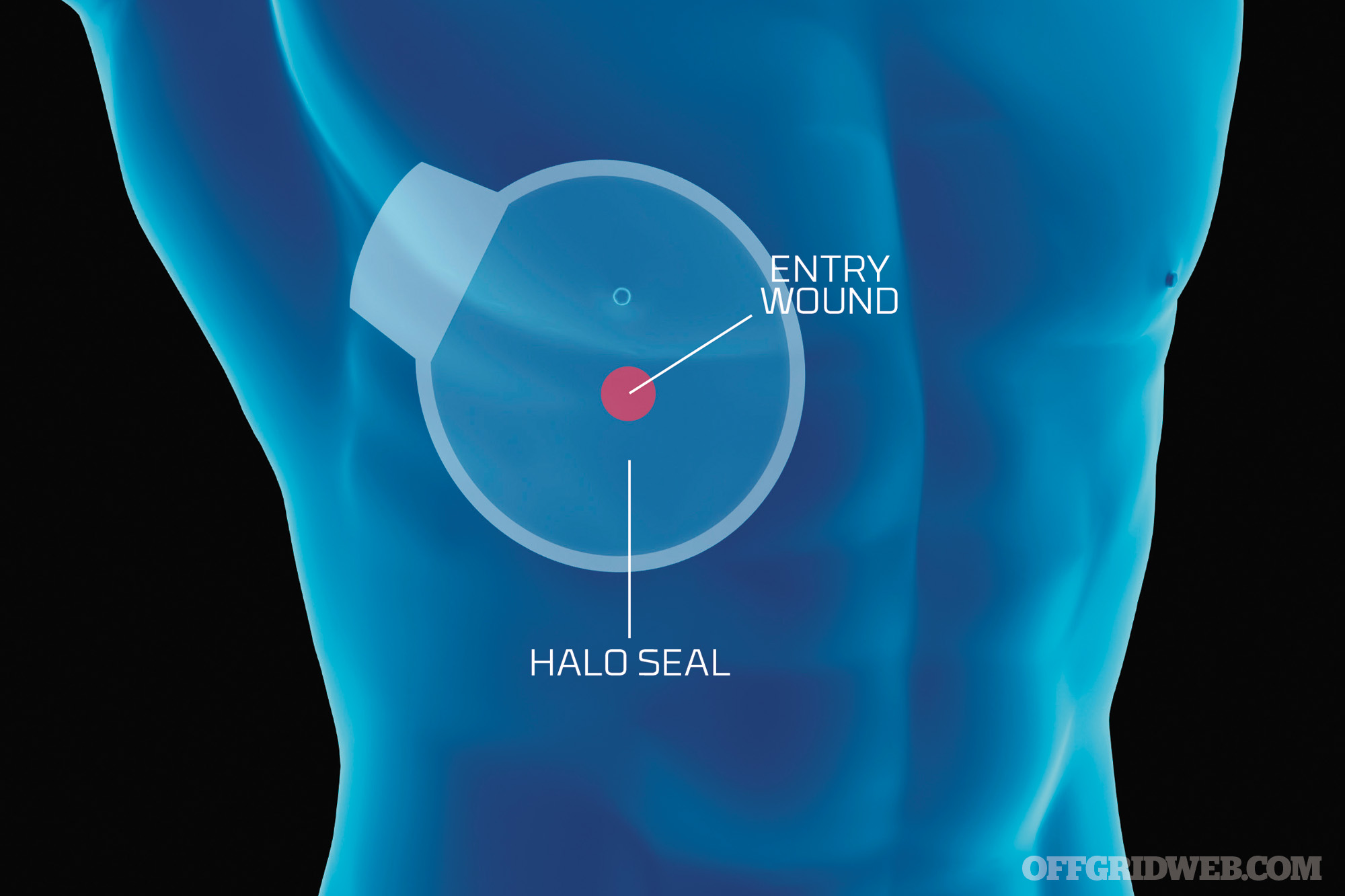
There are two issues that must be addressed with applying a chest seal of some sort. Now, if you do not have a HALO seal, you can use a piece of plastic and tape all sides down. But, if you do have a HALO seal, then make sure you wipe away as much blood as possible first, and then apply the seal. Check the back or the front of the victim, and look for an exit hole, as well. If there is one, apply a chest seal to that area, as well. Once the seals have been applied, you will have to monitor the person and possibly burp or release pressure by lifting up one side of the dressing.

Medical Kits
There are several different types of kits on the market. The first question you need to ask yourself is: What’s my level of training? There is no point in purchasing a trauma surgical kit, if you are not trained how to use it. But, a good blow-out kit, a first-aid kit, a vehicle medical kit, or a home medical kit will be a good thing to have. Actually, it would be best to have several kits listed above in those locations. For more on blow-out kits, take a look at our articles on pocket-sized trauma kits and basic first aid kits.

About the Author
Certified as an EMT-I since 1994, Charles Ferrera spent eight years as an EMT-I on emergency transport units for a fire department. He also has eight years experience as a firefighter and is currently a government contractor for the U.S. State Department High Threat Division. Assigned to Baghdad from 2006-2009, he served in Iraq as a PSS/EMT-I under a U.S. DOS contract. Aside from being an American Heart Basic Life Support instructor for health care providers, he is ACLS Advanced Cardiac Life Support certified and is currently a firearms and tactical medical instructor for Falcon Operations Group (www.falconops.net).

{kind=link}