In This Article
We’ve all been there — you swallow a piece of food that was too big and begin to panic that it won’t go down. For some people, it actually doesn’t go down and starts to become a medical emergency. However, taking too big a bite isn’t the only thing that could cause you to stop breathing. Let’s look at some common airway obstructions and methods to relieve them.
What is the Airway?
Let’s talk about the airway first. It’s the gateway to your respiratory system and can be divided into two sections: the upper airway and the lower airway. The upper airway is comprised of the nasopharynx (nose and throat) and the oropharynx (mouth and throat). The lower airway consists of the larynx (voice box) and trachea (windpipe) before it branches off into the lungs via bronchioles and, finally, alveoli, the small clusters of air sacs where oxygen and carbon dioxide are exchanged via the bloodstream.
What’s an AO?
An airway obstruction is, quite simply, some type of blockage in any part of the respiratory tract that’ll prevent you from being able to get enough oxygen to breathe. The obstruction can be partially or totally obstructed, and it may have various causes.
Types of AO

There are several ways to characterize different types of obstructed airways. One way is based on the location of the obstruction. If you have an upper airway obstruction, you would have an issue with the nasopharynx (nose and throat). A lower airway obstruction would be from your voicebox down to your lungs. A second way is to describe if there’s some air movement or no air movement in the airway. Some are partial, meaning that, while there’s some obstruction, air is still moving in and out of the airway, albeit with varying degrees of difficulty. The size of the obstruction will determine the level of difficulty breathing. In the event of a total, or complete, airway obstruction, the airway is 100-percent stopped up and no air will pass. Once the airway is blocked, respirations stop. This is called respiratory arrest (cessation of breathing). Once respirations stop, oxygenation stops, and, if not relieved quickly, cardiac arrest (cessation of heart activity) will follow.
The third way to characterize an obstruction is based on the timing of the obstruction. Some airway obstructions are acute, meaning they occur suddenly, while others are chronic — a result of issues causing the obstruction to stay in the airway for a long period of time. It might also refer to a blockage that has slowly grown and gradually closed off the airway.
Causes
The most common kind of airway obstruction we think of and see is an acute obstruction, either partial or complete, associated with the inhaling of some type of foreign object — also known as choking. These objects become lodged in the airway and either prevent or completely block off air from entering the lungs, thus preventing adequate oxygenation. The airway could also be blocked off as a result of an illness like epiglottitis, croup, tonsillitis, or any other type of inflammation in the airway, causing acute partial or chronic obstructions.
Airways can also be damaged via heat, as they are made of soft tissue — when injured, they swell quickly, thus compromising the airway. So a person who has inhaled a lot of smoke in a house fire could have some definite airway injuries due to a combination of smoke and heat, which could lead to an acute partial or complete obstruction. A fall, motor vehicle accident, or other traumatic injury could also lead to an acute partial or complete obstructed airway due to bleeding or soft tissue swelling in the airway or by introduction of foreign objects, like teeth, into the airway.
The biggest offender to the stability of the airway seems to be the tongue flopping against the back of the airway in an unconscious individual. When someone is rendered unconscious, the muscles in the body relax. The tongue happens to be a muscle. When it’s relaxed, it can fall against the back of the throat (pharynx) and block the airway. When that happens, we need to act quickly and decisively to open the airway because the longer we wait to get the airway open, the longer the brain is deprived of oxygen.
We can only live for a finite time without that and without suffering brain damage as a result of an anoxic (no oxygen) event. Some chronic disease processes like tumors, asthma, chronic bronchitis, COPD (chronic obstructive pulmonary disease), and emphysema can also cause a progressive narrowing of the airways, limiting the amount of airflow into the lungs. Over time, this can cause a chronic partial obstruction in the airway.
How to Recognize AO
How many of you snore? Yep, that’s a partially — and for some of you at times, a totally — obstructed airway (e.g. obstructive sleep apnea). Snoring is an easy-to-recognize symptom of an obstructed airway. However, depending on the level of obstruction, there are several other signs you can observe. One sign is our respiratory rate. Our normal, adult breathing pattern is fairly steady with a respiratory rate of around 12 to 20 breaths per minute. If we see any deviation from that normal pattern, we need to look closer at what could be causing it. If the patient is breathing more rapidly than normal or shallow, we need to discover the root issue before it gets worse. With partially blocked airways, the patient may be coughing, wheezing, or having other abnormal sounds, like stridor, which is a high pitched or even squeaking sound coming out of the airway.
If the patient can vocalize any sounds, their airway is only partially obstructed. One of the worst things you might see is absolutely no chest rise and fall or unorganized chest wall movements with no sound at all coming from the airway. These are very ominous signs. In a completely obstructed airway, you’d expect to see, in a conscious patient, panic and anxiety with the universal choking signal of putting the hands up to the throat and maybe even mouthing, “I’m choking” or “Help.” If the patient’s oxygen level is dropping, you might also notice a bluish hue in the lips, skin, or nail beds. This is called cyanosis. Finally, if the oxygen levels drop too much, then the brain isn’t getting what it needs — this can lead to unconsciousness in the patient. This is respiratory arrest and, as mentioned earlier, if not relieved, will lead to cardiac arrest and death.
How to Treat AO

When you’re snoring and get elbowed to turn over, you self-correct your own partially obstructed airway by turning over. The offender in this situation is your own tongue. This type of scenario isn’t an emergency. However, if the person isn’t able to correct their own obstruction, it can most certainly turn into one, such as respiratory arrest leading to cardiac arrest. So, how do you treat an airway obstruction? Well, that depends on what’s obstructing the airway.
If the obstruction is an acute partial obstruction, then the patient is moving air and, more than likely, attempting to clear the airway on their own by coughing, which will hopefully dislodge the obstruction.

If it’s an acute complete obstruction such as choking, performing the Heimlich Maneuver is the best option — with no sounds coming from the victim and/or no coughing, the responder wraps their arms around the victim’s waist, slightly above the belly button, makes a fist with one hand, bending the thumb with the knuckle pointed out, covers the fist with the opposite hand, and sharply pulls upward with sets of five abdominal thrusts until the obstruction is relieved. If the airway is partially obstructed due to swelling, either acute or chronic in nature (noted by abnormal sounding respirations, i.e. high pitch, wheezing, etc.), this is a definite emergency and definitive care must be sought out immediately.
Occasionally, you may be alone and have to self-administer abdominal thrusts. In order to do this, you’ll have to find something like a chair or couch to lean over, placing the top of it firmly around your belly button and forcing yourself downward to mimic the same movement of someone else’s hands performing upward abdominal thrusts. The same principle we just mentioned still applies: keep trying in sets of five thrusts until the obstruction is relieved. Different types of airway obstructions will require different interventions, usually based on the severity of the obstruction. This could range from medication inhaled via a nebulizer, placement of a nasal or oral airway, emergent endotracheal intubation, and in worst case scenarios, emergent surgical airway placement.
What to Do if You Can’t Relieve an AO
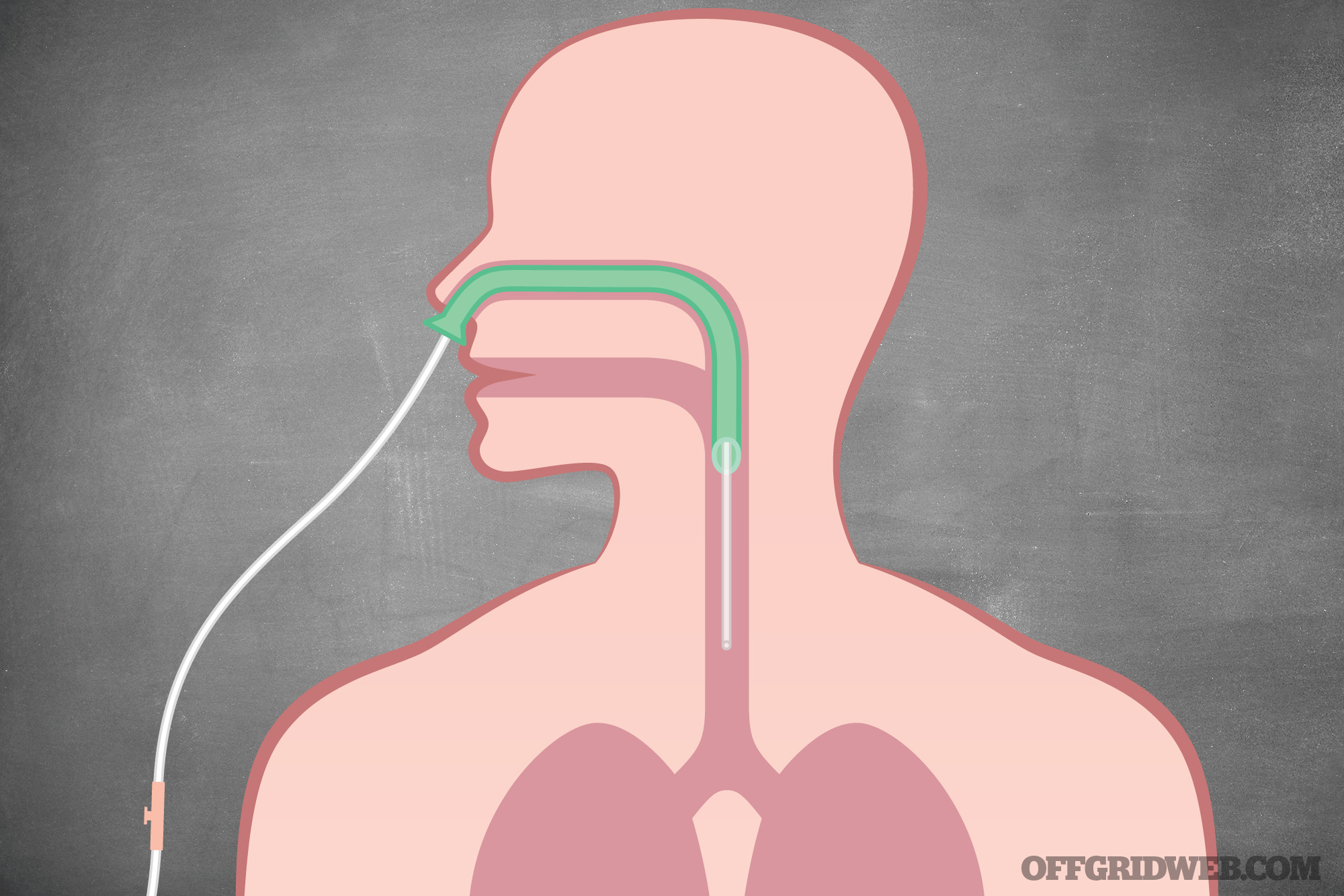
Above: The insertion of a nasopharyngeal airway (NPA) is one method of restoring airflow if the patient’s oropharynx is obstructed. It also offers a pathway for nasal intubation.
In the event the obstruction cannot be removed or the victim becomes unconscious, more actions must be initiated, like CPR. In addition, call 911 for emergency medical services. For more information on CPR and to gain certification, contact your local American Heart Association or American Red Cross office for classes.
If the tongue is the offender and has flopped against the back of the airway, then we can place the affected individual into a recovery position. In this position, the person is rolled onto their side as a unit, with the bottommost arm up and underneath their head to act as support and the uppermost leg acting as a kickstand to support them as the bottommost leg is extended. The victim’s uppermost arm is then placed up in a bent position as a support for their head, while their head is angled toward the ground in an effort to allow gravity to pull the tongue from the back of the throat in order to open the airway.
This allows the person to breathe and also lets blood, saliva, emesis, or anything else to drain out onto the ground rather than going back down the airway, thus creating an aspiration risk. This position can be used if the person still retains a “respiratory drive” or a visible respiratory effort, which can be visualized by the chest rising up and down or the abnormal sounds of respiration from a partially obstructed airway (via the tongue), which in this case would be snoring sounds. This is a very quick and effective method to create a patent (open) airway in someone exhibiting these symptoms while keeping the patient’s airway protected.
Summary
No one wants to be unable to breathe. It’s terrifying. However, understanding what’s going on and how to alleviate it can make the difference between life or death. Seek out the proper training so that if one of these situations occurs, you can be mentally and physically prepared to react. If you act quickly and decisively, everyone involved will breathe a whole lot easier.
About the Author
Kerry Davis is the founder of Dark Angel Medical. He’s a registered nurse who has worked in the critical care and emergency department fields since 2003. Prior to 2003, he was a flight medic in the USAF and worked as a civilian paramedic.

{kind=link}